HOME
Notes on the X Ray appearances of Lobar Collapse
Collapse
or atelectasis is a reduction in the volume of an area of lung.
The X Ray signs of lobar or segmental collapse are described under
three
headings.
1. Changes in density-
(usually a late sign)
(a) The collapsing area may appear denser due to approximation of the
vessels
within it.
(b)
The surrounding lung may appear less dense due to compensatory
emphysema (CE)
usually identified by increased spaces between vessels as compared with
the
other side rather than an obvious increase in blackness. A comparative
vessel
count is often useful.
2. Changes in position- the
hilum , mediastinum and diaphragm may shift towards the site of the
collapse.
Fissures show characteristic movement.
3 Borders
adjacent to collapsed airless lung may be lost.
The following descriptions are of isolated lobar collapse. In practice
there is
often some associated consolidation or pre existing
disease, particularly fibrosis,
which alter appearances.
The appearances described below are only a guide to interpretation in practice.
Total collapse of a lung
gives a whiteout on the affected side due to the airless lung and
movement of
the mediastinum and hemi- diaphragm to fill the space. Ribs on the
affected
side move closer. The other lung shows CE and may appear to cross the
midline.
Rt. upper lobe collapse
The horizontal fissure moves from the horizontal towards the vertical and the upper end of the oblique fissure moves forward.
Fig 1. Fissure
movement in
RUL collapse
AP Lateral.
1.(a) RUL vessels move closer and just before total collapse a density appears alongside the superior mediastinum.
(b) CE in the mid & lower
zones
2. The horizontal fissure
pivots on the hilum. Its lateral and anterior ends moving upwards. The
upper
half of the oblique fissure moves anteriorly . In severe collapse the
two meet
up against the superior mediastinum. Trachea moves to the RT.
RT hilum is elevated and more prominent.
Tenting
may occur
3. In severe collapse the upper
mediastinal border may be lost.
Fig 2. Example of RUL collapse
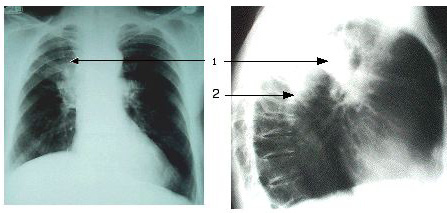
(1)There is crowding of vessels in the RT. upper lobe plus some
increase in
density which the lateral shows to be due to associated consolidation
immediately superior to the oblique fissure in the posterior segment.
The
anterior segment is not consolidated. The consolidation demonstrates
the anterior
position of the oblique fissure. The normally positioned left oblique
fissure
can be seen more posteriorly. (2.)
On the PA it can be seen that the hila are at the same level. Normally
the Rt.
hilum is slightly below the Lft.
Note
Tenting of the diaphragm is often a feature of upper lobe collapse or fibrosis, particularly following TB. If seen as a new feature it may be diagnostic of upper lobe collapse. It is due to the elevation of the hilum pulling on the pulmonary ligament and accessory fissures. The pulmonary ligament is a strand of fibrous tissue between the hilum and the diaphragm.
Left
Upper Lobe Collapse
Oblique fissure moves forwards
(straight arrows) and
comes to lie close to the anterior
chest wall. In severe collapse the
anterior part of
the lobe moves posteriorly away
from the anterior chest wall. The lower lobe then comes over the top of
the
collapsed lobe (curved arrow) and comes to lie against the anterior
chest wall.
On the frontal view the fissure is not seen but the collapsed lung may
become
evident against the upper mediastinum.
FIG 3 Fissure movement in LUL collapse
1. (a) The vessels in the LUL approximate and a density appears
around the
aortic knuckle (PA). The anterior part of the chest becomes
increasingly denser
(lat).
(b)
CE
in the LLL.
2. The fissure moves as shown in Fig 3. Trachea moves left. As the LLL
expands
the diaphragm and the L hilum may elevate, tenting may occur.
3. As the lobe collapses it rests against the aortic knuckle which lies
anteriorly. As it loses air and becomes dense the aortic knuckle
disappears. If
the collapse advances further the knuckle may be seen again outlined
against
the lower lobe.
FIG
4
An
example of advanced LUL collapse. The collapsed lobe is closing down
onto the
hilum, becoming denser and causing the veil -like shadowing
around the hilum. Note that there is no shift of
the mediastinum, trachea, hemi diaphragm or hilum.
Nor is there any obvious compensatory emphysema. There is no
pre existing lung disease and the lower lobe is sufficiently large and
flexible to fill the
available space. It is large enough to
have come round medial to and
above the collapsing lobe causing the lucency around the aortic knuckle
and
allowing this structure to be clearly seen.
Right
Middle Lobe Collapse
The horizontal fissure & lower half of the oblique fissure
approximate.
The horizontal fissure is the more mobile. The collapsed lobe comes to
lie
against the heart border.
Fig 5 fissure movement in middle lobe collapse
1 Because the lobe is small CE is rarely seen. There may be a vague
density
against the heart border (PA)
better seen on the Lateral as a clear wedge shaped opacity.
2 Fissure movement as described. Best seen on the lateral. On a PA film if the horizontal fissure is not seen
any other changes may not be recognised.
3 In the late stages the RT. heart border may be lost.
Fig 6 Example of middle lobe collapse
There is loss of the right heart border. The horizontal fissure cannot
be seen.
On the lateral the horizontal fissure and the oblique fissure have
approximated
to each other leaving the middle lobe as a linear density overlying the
heart
shadow (arrowed).
Lower
Lobe Collapse
The pattern is similar on both sides. The oblique fissure moves
backwards
and medially. The fully collapsed
lobe becomes a wedge of tissue lying up against the posterior
mediastinum. The
middle and upper lobes expand to fill the space lateral and anterior to
the collapsing lobe.
Fig 7 fissure movement in lower lobe collapse
1.(a)
As the lobe moves posteriorly it
becomes increasingly dense on the Lat. On the AP view it may be seen as
a wedge
shape (through the heart shadow on the left).
(b) CE in the RUL.
2. The oblique fissure moves backwards. On the Rt the horizontal fissure may move in a similar way to RML collapse but the lung underneath it becomes less rather than more dense. There is movement of the heart shadow towards the side of the collapse and the hemi-diaphragm may elevate especially if there is pre-existing lung disease limiting the CE. The hilum becomes depressed.
1.There
is a triangular opacity behind the heart on the left.
CE could be identified on the left by comparing the number of vessels
on the
two sides.
2 The heart shadow has moved slightly
to the left.
The left hilum is depressed.
On
the
lateral little in the way of density change can be identified.
One oblique fissure has moved backwards slightly and can be seen behind
the
hilum. The other can still be seen in front of the hilum (double
arrow). The
posterior part of the left diaphragm cannot be identified although the
stomach
bubble (arrow) shows you where it should be. Its anterior part can be
identified in front of the little diaphragmatic "tent" near to the
inferior insertion of the oblique fissure. The right hemi-diaphragm can
be
clearly seen. This must mean that there is a considerable increase in
the
density of the collapsing lung possibly with some associated
consolidation.
Lingular
collapse
Often involved in upper lobe collapse, but the lingula may collapse
on its
own. Features are identical to RML collapse except that the horizontal
fissure
is not there to help you. On the frontal view the only evidence may be
a subtle
loss of the Lft. heart border.